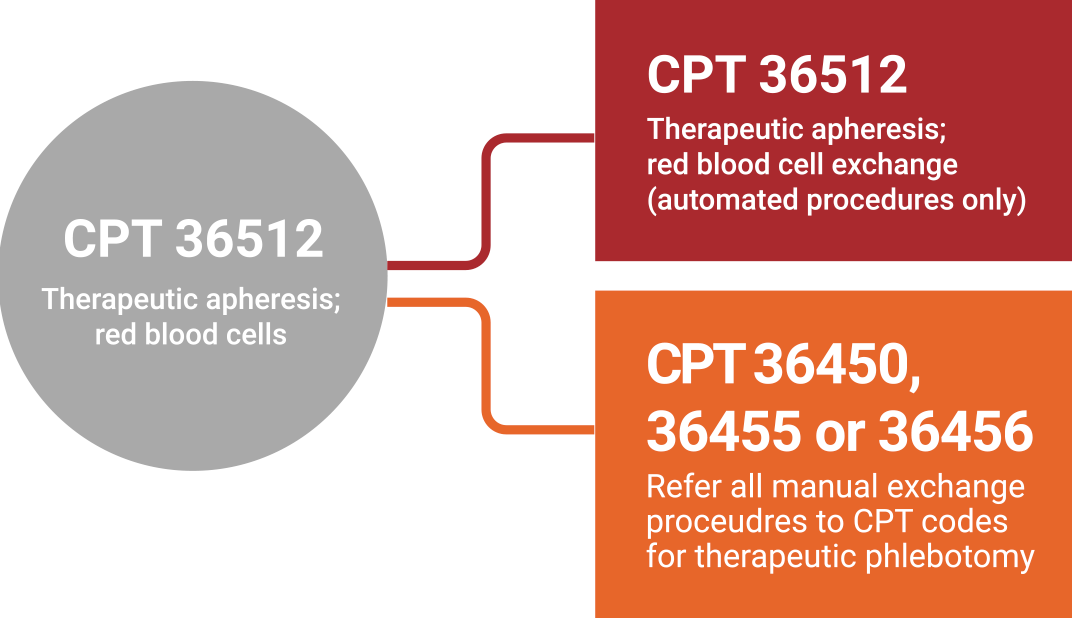
Not all transfusion therapies are the same, and neither is their coding. Starting January 1, 2021, automated red blood cell exchange (RBCX) will have a distinct CPT code.
Manual red blood cell exchange procedures will be coded to therapeutic phlebotomy codes. Make
sure you are ready for this change in transfusion coding.
Differences in Transfusion Therapies for Patients With Sickle Cell Disease

“I really didn’t find anything that was
effective for keeping me away from
having crises except for automated
RBCX.”
Rona Wiggins, patient with sickle cell disease
Rona Wiggins, patient with sickle cell disease
Automated RBCX
Procedure code
CPT 36512
Iron-neutral procedure 1
Yes
Procedure time 1
110 minutes
Number of procedures1
8.5 per year
Manual Transfusion Therapies
Procedure code
CPT 36450, 36455 or 36456
Iron-neutral procedure 1
Yes
Procedure time 1
245 minutes
Number of procedures1
12 per year
Reimbursement differs by therapy.
Remember to use the appropriate CPT procedure code for the transfusion therapy that is right for your patient. Effective January 1, 2021, the average Medicare OPPS (Outpatient Prospective Payment System) reimbursement for Automated RBCX will be $1,363.16.2,*
Remember to use the appropriate CPT procedure code for the transfusion therapy that is right for your patient. Effective January 1, 2021, the average Medicare OPPS (Outpatient Prospective Payment System) reimbursement for Automated RBCX will be $1,363.16.2,*
*Terumo Blood and Cell Technologies provides this information for your convenience only. It does not constitute legal advice or a recommendation regarding clinical practice. Information provided is gathered from third-party sources and is subject to change without notice due to frequently changing laws, rules, and regulations. The provider has the responsibility to determine medical necessity and to submit appropriate codes and charges for care provided. Terumo Blood and Cell Technologies makes no guarantee that the use of this information will prevent differences of opinion or disputes with Medicare or other payers as to the correct form of billing or the amount that will be paid to providers of service. Please contact your Medicare contractor, other payers, reimbursement specialists, and/or legal counsel for interpretation of coding, coverage, and payment policies. This document provides assistance for FDA-approved or cleared indications. Where reimbursement is sought for use of a product that may be inconsistent with, or not expressly specified in, the FDA-cleared or approved labeling (e.g., instructions for use or operator’s manual), consult with your billing advisors or payers on handling such billing issues. Some payers may have policies that make it inappropriate to submit claims for such items or related service.

